Vaping FAQs
The basics
The main purpose of tobacco harm reduction is to reduce (not necessarily eliminate) the harm from smoking. The aim is not to stop nicotine as nicotine causes little harm. Tobacco harm reduction involves encouraging smokers to switch from high-risk combustible (burnable) cigarettes to a lower-risk nicotine alternative such as vaping.
Complete cessation of all tobacco and nicotine consumption is always the ideal goal. However, a large proportion of smokers are unable or unwilling to quit, therefore remaining at high risk of smoking-related death and illness. THR aims to reduce the health risks in continuing smokers by switching from combustible tobacco to lower-risk smokeless nicotine alternatives. Smokeless products are not risk-free but are much safer than smoking.
Reduced-risk products include vaping (using an e-cigarette), Swedish snus (small pouches of special tobacco placed under the upper lip), nicotine pouches (similar to snus but without tobacco) and heated tobacco products (which heat tobacco without burning it).
Burning tobacco causes almost all the harm from smoking. It releases over 7,000 chemicals, tars, carbon monoxide, other toxic gases and solid particles.
Safer nicotine products can complement (not replace) traditional tobacco control strategies which target complete quitting.
Tobacco harm reduction is no different to other harm reduction strategies which are generally very effective and widely accepted. These include methadone for heroin users, clean needle exchange programs and even car seat belts.
Tobacco harm reduction is one of the three pillars of Australia’s National Tobacco Strategy. One objective of the NTS is to “reduce harm associated with continuing use of tobacco and nicotine products” (p11).Australia is legally obligated to support tobacco harm reduction as a signatory to the World Health Organisation Framework Convention on Tobacco Control.
The FCTC provides an obligation on governments to not only allow reduced-risk products but actively promote them as part of implementing their tobacco control policies. Currently Australia is in breach of its international obligations as no harm reduction strategies are supported in practice.
Vaping is a less harmful alternative for adult smokers who are often unable to quit smoking on their own or with other methods. Vaping delivers nicotine and mimics the familiar hand-to-mouth action and sensations of smoking.
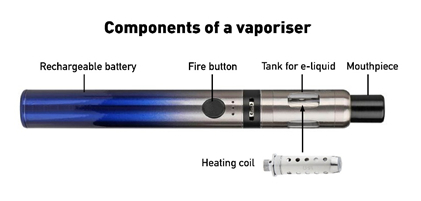
Nicotine vaporisers (e-cigarettes) heat a liquid nicotine solution into an aerosol which is inhaled and exhaled as a visible mist. This is known as ‘vaping’.
All vaporisers consist of a battery (usually rechargeable), a tank or reservoir to hold the e-liquid and a coil or heating element to heat the liquid to create the vapour.
As there is no tobacco and no combustion, almost all the toxic chemicals in smoke are absent from vapour. Those that are still present are in far lower doses than in tobacco smoke.
Some smokers use vaping for a short time to quit tobacco smoking and then cease vaping. Others continue vaping long-term to prevent relapse to smoking. Some smokers experiment with vaping without intending to quit but then ‘accidentally’ quit.
Vaping should not be used by non-smokers including young people who don’t smoke.
Most people who take up vaping are smokers trying to reduce their risk of harm from smoking.
In Australia in 2019, smokers gave the following reasons for taking up vaping (could select more than one response) according to the 2019 National Drug Strategy Household Survey:
- To quit smoking 44%
- To reduce smoking 32%
- To avoid relapse to smoking 23%
- Because they are less harmful 27%
- They are cheaper 23%
- 44% of smokers said curiosity was a factor in their decision to try vaping
In 2019, 520,000 Australians aged 14 and older, or 2.5% of the population, were ‘current’ vapers ie had vaped at least once in the past 12 months (2019 NDSHS).
This was made up of
- 281,300 current smokers (“dual users”)
- 198,000 ex-smokers
- 43,000 never-smokers
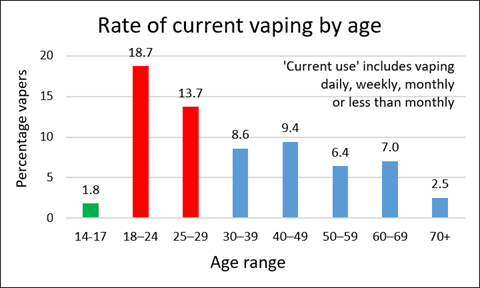
Vaping rates were highest in young adults and gradually decreased with age. Rates in teens are very low.
Men are slightly more likely to vape than women.
The number of vapers has more than doubled since 2016 when 1.2% of the population (14+) or 238,000 people were current vapers. (2016 NDSHS) Vaping rates in Australia are low by international standards due to legal restrictions and opposition from medical and health organisations, but are now starting to rapidly rise.
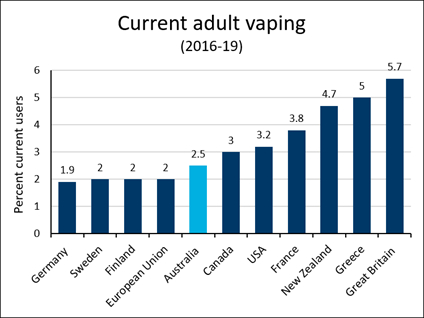
References: Australia NDSHS 2019; Sweden Hedman 2018; Germany Kotz 2018; Finland Ruokolainen2017; EU Eurobarometer 458 2017; US Dai, JAMA NHIS 2019; Canada CTADS 2017; NZ Health Survey 2018/19; France Pasquereau 2018; Greece Farsalinos 2018; GB Office of National Statistics 2018
It is possible to vape legally in Australia with a nicotine prescription from a doctor. However, most vapers in Australia do not have a prescription and are breaking the law. Australia is the only western democracy to effectively ban the sale and use of nicotine liquid for vaping.
Nicotine is classified as a Schedule 7 ‘dangerous poison’ in the Poisons Standard, like arsenic and strychnine. However, at present, people can legally import nicotine from overseas to help them quit or reduce smoking if they have a prescription. Under the Therapeutic Goods Administration (TGA) Personal Importation Scheme, 3 months’ supply can be imported at a time for personal use.
There are severe penalties (up to $45,000 and up to two years jail) for using or possessing liquid nicotine unless it is prescribed by a doctor to help you quit or cut down smoking. Less than 1-2% of Australians who vape have a prescription.
State and Territory laws regulate issues such as sale, use in public places, age limits on sale, display and promotion of vaporisers.
Reading
Vaping and the law. ATHRA
Safety and health
There is overwhelming scientific agreement that vaping is far less harmful than smoking. Vaping does not produce smoke. It is the 7,000 toxic chemicals in smoke released from burning tobacco which cause almost all the deaths and disease from smoking.
In contrast, e-cigarettes heat a liquid into an aerosol, without tobacco, combustion or smoke. Some potentially harmful toxins are present in aerosol but at much lower levels than in cigarette smoke.
According to the UK Royal College of Physicians:
“Although it is not possible to precisely quantify the long-term health risks associated with e-cigarettes, the available data suggest that they are unlikely to exceed 5% of those associated with smoked tobacco products, and may well be substantially lower than this figure.”
A comprehensive review by Public Health England concluded:
“While vaping may not be 100% safe, most of the chemicals causing smoking-related disease are absent and the chemicals which are present pose limited danger.”
A review by the US National Academies of Sciences, Engineering and Medicine concluded:
“There is substantial evidence that completely switching from regular use of combustible tobacco cigarettes to e-cigarettes results in reduced short-term adverse health outcomes in several organ systems.”
Numerous studies have also shown substantial reductions in biomarkers (toxins in the blood, saliva and urine) of tobacco smokers who have switched to vaping.
Yes. This estimate is based on comprehensive, independent reviews of the scientific evidence by both Public Health England and the UK Royal College of Physicians. It is a reasonable guide to the risk from vaping compared to smoking.
The Royal College of Physicians put it this way:
“Although it is not possible to precisely quantify the long-term health risks associated with e-cigarettes, the available data suggest that they are unlikely to exceed 5% of those associated with smoked tobacco products, and may well be substantially lower than this figure”
Of course, the exact figure doesn’t really matter, but saying the risk of vaping is probably less than 5% of smoking helps to communicate a ballpark for the level of risk so smokers can make an informed choice. Just saying vaping is ‘less harmful’ is too vague. That could be 30%, 60%, or maybe even 99% less harmful.
The ”95% safer” figure is based on the following evidence
- Most of the harmful toxins in smoke are completely absent from vapour. Those that are present are at much lower concentrations, mostly at levels below 1% of what they are in smoke. If the toxins are much lower, the health risks will be much lower.
- When smokers switch to vaping, levels of toxins and carcinogens measured in the blood, saliva and urine (‘biomarkers’) are substantially lower and for many toxins are the same as for a non-smoker.
- There are substantial health improvements in smokers who switch to vaping. Risk of a heart attack reduces, the blood pressure falls, asthma and COPD (emphysema) improve and smokers often say they just feel a lot better after switching.
- The risk of cancer from vaping has been independently estimated to be <0.5% of the risk from smoking.
- After 15 years of vaping nicotine in dozens of countries, there has not been one death. Serious health effects are extremely rare.
In spite of what many people think, nicotine does not cause cancer and the cancer risk from vaping is only a tiny fraction of the risk from smoking.
The overall cancer risk from vaping nicotine is estimated to be <0.5% of the risk from smoking. The lung cancer risk has been estimated to be 50,000 times less than from traditional cigarette smoking. Switching from smoking to vaping dramatically reduces the risk of developing cancer.
Tobacco smoke contains at least 70 known carcinogens (cancer-causing chemicals). These are either absent from vapour or are present at very low levels.
The highest-ranking carcinogens in cigarette smoke, 1,3-butadiene and acrylonitrile (which account for more than three-quarters of the cancer risk from smoking) are almost completely absent from vapour.
There is also a dramatic reduction in cancer-causing chemicals in the saliva and urine of vapers (biomarkers) compared to smokers.
Unlike second-hand smoke, the risk to bystanders from passive vaping appears to be minimal.
According to Public Health England’s review in 2018, “to date there have been no identified health risks of passive vaping to bystanders”. The report of the Royal College of Physicians in 2016 stated “There is, so far, no direct evidence that such passive exposure is likely to cause significant harm.”
This is because the vaper absorbs most of the inhaled aerosol. Less than 10% of the chemicals are exhaled and they are at very low levels in the air. There is also no ‘side-stream’ vapour, while side-stream smoke accounts for at least 80% of second-hand smoke from a cigarette.
Furthermore, the liquid aerosol droplets from vapour evaporate and disperse in seconds, much more quickly than the solid particles in smoke, reducing risk further.
Based on the carcinogens in second-hand vapour and the estimated doses, the cancer risk for passive smokers was estimated to be five orders of magnitude (50,000x) greater than for passive vapers.
Nicotine is a relatively benign drug. Although it is addictive, it presents very little risk to the user and even has some significant beneficial effects.
Because of its association with smoking, many people incorrectly believe it is the harmful ingredient in tobacco smoke. However many independent expert bodies disagree:
- UK Royal College of Physicians, “Use of nicotine alone, in the doses used by smokers, represents little if any hazard to the user” p. 125.
- The Royal Society for Public Health has concluded that nicotine is a mild recreational stimulant and is “no more harmful to health than caffeine”.
- Public Health England “nicotine use per se represents minimal risk of serious harm to physical health and that its addictiveness depends on how it is administered”
Nicotine does not cause cancer or lung disease and only has a minor role in cardiovascular health.
The vast majority of harm from smoking comes from tar, carbon monoxide, toxic gases and solid particles released by burning tobacco, not from the nicotine.
Nicotine has mild effects such as temporarily increasing the pulse and blood pressure and narrowing the blood vessels. It can impair wound healing and raise blood glucose levels.
Long-term use of nicotine is regarded as low risk, based on decades of use of Swedish snus which releases high levels of nicotine and nicotine replacement therapy.
The addictiveness of nicotine alone is also overrated. There are other ingredients in tobacco smoke which make nicotine more addictive (monoamine oxidase inhibitors). Cigarettes also deliver nicotine very quickly which increases its addictiveness. However, outside of tobacco smoke, nicotine is far less addictive. For example, nicotine gum and patches have very low risk of dependence but are used long-term by some ex-smokers to prevent relapse. The behavioural, sensory and social aspects of smoking also enhance its addictiveness.
Benefits from nicotine
Nicotine has many positive effects such as:
- Enhanced attention and concentration, arousal, fine motor skills and working memory [ref]
- Pleasure and relief of anxiety and depression [ref]
- Positive effects on Parkinson’s disease, schizophrenia, ulcerative colitis and attention deficit disorder
- Weight control
- Pain relief
Reading
Niaura R. Re-thinking nicotine and its effects. Truth Initiative 2016
It is beyond reasonable doubt that the risks from vaping nicotine are much less than those of smoking which kills up to 2 in 3 long-term users.
Like all new products, the precise long-term health effects of vaping nicotine have yet to be established. However, we already have a lot of information about the ingredients of vapour, biomarkers (toxins in urine and saliva) and over 15 years of real-world experience and scientific studies to guide us. There are now an estimated 68 million people vaping in dozens of countries.
The Royal College of Physicians estimates the long-term risk is likely to be no more than 5% of the risk of smoking.
Studies so far show no cause for concern in people vaping after stopping smoking for up to 2 years. One study of four years and another of five years duration have not raised health concerns.
Some opponents argue that we should wait another 30 years to be sure about long-term risk. However, this is a double standard only applied to vaping and not used for any other medicine or treatment.
As with any new product, it is possible that some harms may emerge over time and ongoing monitoring of vaping should continue for any new side-effects. However, it may never be possible to completely separate the effects of smoking from those due to vaping as almost all regular vapers are former smokers.
If cigarettes were invented today, we would know very quickly that they were very harmful.
We know much more today about chemistry, toxicology, physiology and causes of disease than when cigarettes were introduced over a century ago. We have a much greater understanding of the toxic effects of most chemicals and can assess them against occupational and environmental health and safety standards.
The scientific method, analytical techniques and equipment are far superior to that available in the past.
No. This condition was not caused by nicotine vaping.
In 2019, there was an outbreak of serious lung injury (EVALI) in the US in people who had recently vaped. This condition has now been clearly associated with black-market cannabis oils contaminated with Vitamin E Acetate, purchased from street dealers.
Not a single case has been linked to commercial nicotine vaping to stop or reduce smoking.
No. There is no evidence that vaping nicotine causes this condition and there has not been a single case linked to vaping.
‘Popcorn lung’ (bronchiolitis obliterans) is a serious, but rare lung disease first detected in popcorn factory workers. It was linked to very high levels of ‘diacetyl’ which is used to create a buttery flavour.
Some earlier e-liquids contained diacetyl, however the levels found in vapour were hundreds of times lower than in cigarette smoke and there has never been a case of bronchiolitis obliterans due to smoking or vaping. Diacetyl is now rarely used.
Reading
1. New Study Finds that Average Diacetyl Exposure from Vaping is 750 Times Lower than from Smoking. Prof Michael Siegel
2. Does vaping cause popcorn lung? Cancer Research UK
3. Clearing up some myths around e-cigarettes. Public Health England
There is currently little evidence on the safety of vaping in pregnancy however it is certain to be safer than smoking. Most of the harmful chemicals in smoke are absent or dramatically reduced in vapour.
Nicotine has been linked to harmful effects on the fetus in animal studies. However, there is no evidence that these findings apply to humans.
Nicotine replacement products such as patches, gums and lozenges are approved for use in pregnancy in Australia. Human studies have not shown any clear harms from their use, such as stillbirth, premature birth, low birthweight, admissions to neonatal intensive care, caesarean section, congenital abnormalities or neonatal death.
Nicotine may not be completely safe for the pregnant mother and fetus, but it is always safer than smoking.
The use of vaping in pregnancy is endorsed by an important expert group in the UK, the Smoking in Pregnancy Challenge Group, a partnership between the Royal College of Midwives, the Royal College of Obstetricians and Gynaecologists and the Royal College of Paediatrics and Child Health.
The Challenge Group provides the following advice to midwives:
“Very little research exists regarding the safety of using e-cigarettes (vaping) during pregnancy, however evidence from adult smokers in general suggests that they are likely to be significantly less harmful to a pregnant woman and her baby than continuing to smoke.”
The UK Royal College of Midwives 2019 Position Statement on quitting in pregnancy states:
“E-cigarettes contain some toxins, but at far lower levels than found in tobacco smoke. If a pregnant woman who has been smoking chooses to use an e-cigarette (vaping) and it helps her to quit smoking and stay smokefree, she should be supported to do so.”
Although it is not risk-free, vaping may have a role as a substitute for pregnant women who are unable to quit smoking with other methods. It should not be used by women who do not smoke.
Reading
1. Use of electronic cigarettes before, during and after pregnancy. A guide for maternity and other healthcare professionals. Smoking in Pregnancy Challenge Group 2020
2. Position Statement. Support to Quit Smoking in Pregnancy. The Royal College of Midwives. 2019
Almost all vapers are already dependent on nicotine from past smoking but have transferred their nicotine dependence to a much safer product. Smokers who switch to vaping become less dependent and find it easier to quit vaping when they are ready to try.
Smoking is particularly addictive because it delivers high levels of nicotine very rapidly to the brain. Vaping releases nicotine more slowly and generally to lower levels. However, some vaping devices can deliver nicotine in a similar speed and dose to smoking.
Smoke also contains other chemicals that make nicotine more addictive eg monoamine oxidase inhibitors. These chemicals are not present in vapour.
Nicotine dependence from vaping is rare in young people who have never previously smoked. In the US, less than 4% of young never-smokers who vaped reported symptoms of addiction to vaping.
Many people do not regard dependence on nicotine from vaping as a problem. Vaping nicotine has many beneficial and enjoyable effects and nicotine is a relatively benign substance in the doses used.
Accidental poisoning from nicotine e-liquid is rare especially when compared to poisoning from other chemicals and medicines. Ingestion of nicotine is usually followed by intense vomiting and most cases result in a mild outcome. There have been four deaths in children from nicotine poisoning reported globally in the last 15 years.
The Australian Poisons Information Centres reported on exposure to nicotine e-liquid. There were 202 cases over 7 years from 2009-2016, of which 36% were children. Most patients only had mild symptoms with 12 having moderate symptoms, usually gastrointestinal. There were no cases with serious side-effects and no deaths.
The Victorian Poisons Information Centre reported low rates of exposure to liquid nicotine in 2018 and 2019. The number of cases referred for treatment was 14 in 2018 and 15 in 2019. The claim by the Health Minister (19 June 2020) that nicotine poisoning had doubled during this time period is incorrect.
There has been one death in Australia from accidental nicotine liquid poisoning. In May 2018, an 18-month old child died after drinking from an open (non-childproof) bottle of imported concentrated nicotine (100mg/ml) when the mother was mixing the nicotine with locally purchased flavours. This tragic case underlines the importance of regulating low-concentrations of nicotine liquid for legal sale, so it is available in child-proof containers with warning labels.
Three other accidental child deaths have been reported since 2013: one each in Israel, Korea and the US.
Accidental nicotine poisoning is rare in other western countries such as the United States, United Kingdom and Canada. Most cases are mild and self-limiting.
According to a review by Public Health England, the risks of ingestion of e-liquids appear comparable to similar potentially poisonous household substances.
Exposure to poisons is widespread in society and is associated with many products from which society benefits, such as bleach and laundry detergents. These are managed by common-sense, warning labels and child resistant containers – not by bans.
Rechargeable lithium ion batteries in vaporisers can malfunction (“thermal runaway”) resulting in thermal and chemical burns and traumatic injuries. Fortunately, these incidents are very rare but are increasing as vaping becomes more popular.
Malfunctions of this type do not occur in the popular beginner models, ie sealed pod devices and pen-style models in which the battery is built-in and not removable. Most problems occur with loose, replaceable batteries and ‘mechanical mods’ used by some experienced users.
Lithium ion battery malfunctions also occur in other electrical devices such as mobile phones and laptops.
Tobacco cigarettes remain the biggest cause of fatal house fires. According to the London Fire Brigade “Switching from smoking tobacco to vaping can greatly reduce the risk of dying in a fire”.
Most incidents could be prevented by user education eg
- Plastic storage cases to avoid contact of loose batteries with keys or coins,
- The use of quality batteries
- Avoiding “mechanical mods” which lack safety features
- Using a compatible charger
- Replacing damaged batteries
- Battery regulation and improved electrical safety standards
Quitting Smoking
There is compelling evidence that vaping helps smokers quit. It is more effective than nicotine replacement therapy (patches, gums, lozenges) and is arguably the most effective quitting aid available.
Randomised controlled trials (RCTs) show that vaping helps smokers quit in a controlled environment more effectively than nicotine patches and gums (NRT). A study from the UK found that vaping was almost twice as effective as NRT after 12 months. Another large study from New Zealand showed that adding vaping to a nicotine patch tripled the success rate after 6 months compared to using the patch alone.
Three meta-analyses of the best quality RCTs (pooling the data from all studies) here, here and here all concluded that vaping was 70% more effective than nicotine replacement as a quitting aid. RCTs are likely to underestimate the effectiveness of vaping in the real world (see #3).
The better quality observational studies show that vaping increases quitting in the real world.
Large population studies in the United States and the United Kingdom have also found that smokers who use vaping to quit have significantly higher quit rates than those who do not. Daily vapers were 3–8 times more likely to quit than smokers who did not vape.
It is also noteworthy that the rate of decline in smoking in both the United States and United Kingdom has accelerated since vaping nicotine became popular around 2013. It is highly likely that vaping is the major contributing factor to this rapid decline.
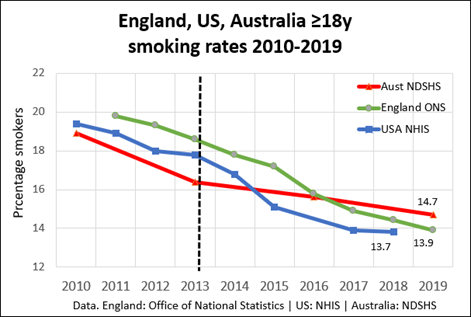
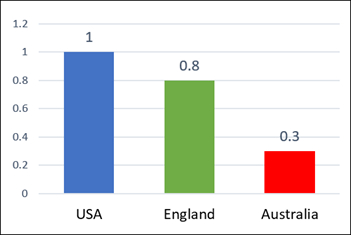
The adult smoking rate in the US and UK has declined 3 times faster than in Australia since 2013: Australia 0.3% per year, compared to 1% per year in the US (2013-2018) and 0.8% per year in England (2013-2019).
Further support for the scientific evidence for the effectiveness of vaping comes from the thousands of testimonials of former smokers who now vape, for example here and those who no longer smoke or vape. While these testimonials are not scientific evidence, they should not be ignored.
Reading
Vaping nicotine is now the most popular quitting aid in Australia and in many countries where it is readily available.
In 2019, 22% of Australian smokers used vaping to help them quit (8%) or reduce (14%) smoking. The next most popular quitting aid was nicotine replacement therapy (17%), followed by smoking cessation pills (6%), quit smoking apps (5%) and Quitline (2%).
Vaping devices are also the most popular quitting aid in the United Kingdom, the United States and the European Union.
Vaping devices were used in 32% of quit attempts In England in 2019 and in 27% of quit attempts in France.
Because of its combined popularity and effectiveness, the public health impact of vaping is even greater.
Only short-term use is recommended but long-term vaping is safer than relapsing to smoking.
It is recommended that smokers should try to stop vaping once they have successfully quit smoking. However, for many former smokers, relapse to smoking is a constant fear. Research suggests that vaping may play an important role in preventing relapse. Vaping can act as a substitute for smoking behaviour to help cope with urges to smoke.
The small health risk from continuing to vape is minor compared to the harm from relapsing to smoking.
Smokers vary in the length of time they continue to vape after switching from smoking. Most have also quit vaping within a couple of years. Only a small proportion continue vaping for many years.
Youth vaping
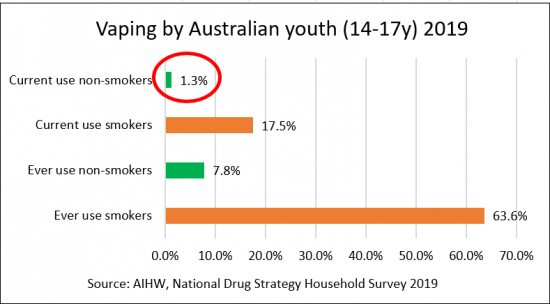
No. Youth vaping rates are low and most use is experimental and infrequent. Regular vaping is largely confined to smokers or ex-smokers and is rare in never-smokers.
In Australia in 2019, only 1.8% of 14-17 year olds had vaped once or more in the last 12 months, according to the National Drug Strategy Household Survey. Vaping is much more common in those who were already smokers with 17.5% trying vaping. Only 1.3% of non-smokers had vaped.
Regular vaping is rare in youth who have not smoked. In Australia in 2017, only 0.3% of 12–17 year old never-smokers had vaped on 3 or more days in the last month, in the Australian Secondary Students’ use of Alcohol and Drug Survey.
Similar low rates of regular vaping by non-smokers are found in the United Kingdom (0.1-0.5%), New Zealand (1.1%) and the United States (0.4%).
Vaping rates in youth are higher in the US than most other countries but are now declining. Most vaping is experimental, transient and infrequent and is mainly by current or past smokers. Regular vaping by non-smokers is rare. Many US youth vape without nicotine.
The key questions for public health are whether non-smokers are taking up regular vaping and whether smoking rates are increasing. The results are very reassuring.
Vaping rates by high schoolers declined by 30% from 2018 to 2019 (27.5% to 19.6%). There was also a 58% decline in vaping by middle schoolers (from 10.5% to 4.4%). Only some were using nicotine. Many young people in the US are vaping cannabis and flavours instead.
Most youth who try vaping are already smokers. In the US, 85% of current smokers aged 12–15 years had not vaped before they began to smoke cigarettes. Some of these are smokers who have switched to vaping to quit smoking.
Regular vaping by US non-smoking youth is rare. Only 0.4% of never-smokers vaped regularly (≥20 days in the last 30 days). Nicotine dependence is rare in never-smoking young people who vape. In 2018, less than 4% of never-smokers reported symptoms of nicotine dependence.
The decline in youth smoking rates in the US accelerated 2-4 times after 2014 when vaping became popular. US youth smoking rates (12th grade) also fell by an unprecedented 30% from 2018 to 2019 (8.1% to 5.7%). This rapid decline is much faster than in Australia where vaping is banned and suggests that vaping is diverting youth from smoking and is acting as a gateway out of smoking.
After analysing the data in detail, West concluded
“Data from the NYTS [National Youth Tobacco Survey] do not support claims of a new epidemic of nicotine addiction stemming from use of e-cigarettes, nor concerns that declines in youth tobacco addiction stand to be reversed after years of progress”
There is an epidemic of ‘moral panic’ in the US about vaping, but no ‘epidemic’ of youth vaping.
Although teens who try vaping are more likely to try smoking later, there is no good evidence that vaping actually CAUSES them to take up smoking if they would not already have done so.
A more plausible explanation is that young people who experiment with risky behaviours such as vaping are more likely to try other risky behaviours such as smoking, alcohol, cannabis and other drugs (‘common liability’).
To the contrary, the evidence suggests that vaping is diverting some young people from smoking. In countries where vaping is readily available, the decline in youth smoking has accelerated since vaping became popular. In the US, smoking rates in high schoolers fell by an unprecedented 30% in 2018 in spite of high levels of experimentation with vaping. This and other evidence suggest that some adolescents who would otherwise have smoked may try vaping as a less harmful alternative to smoking and not progress to smoking.
Smoking more often precedes vaping than vice versa, i.e. most youths who tried vaping are already cigarette smokers or have previously experimented with cigarette smoking. In the 2017 Australian Secondary Students’ Alcohol and Drug Survey, two in three 12–17 year-olds who had ever vaped had first smoked. In studies in the US and UK, around 85% of young people report vaping before smoking.
Reading
Restricting flavours will have little effect on youth vaping but will reduce the appeal of vaping to adult smokers.
Flavours are an integral part of vaping which makes it more appealing to adult smokers as an alternative to smoking. Flavours play an important role in the initiation of vaping for current smokers and in reducing the likelihood of relapse. Flavours are used in nicotine replacement products for this reason. Nicorette gum is available in Australia in fruit, mint, spearmint and icy mint flavours and research shows that flavoured nicotine gum enhances appeal and improves compliance.
Flavours increase quit rates from vaping compared to non-flavoured or tobacco flavours.
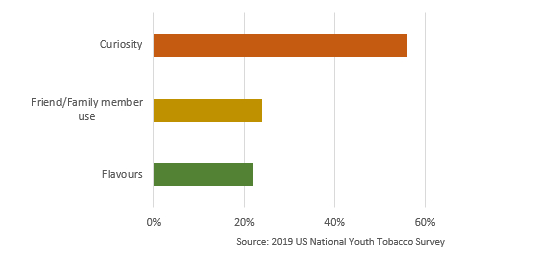
Flavours are not the primary reason for youth experimentation with vaping in Australia or the US. For example, in the US in 2019 they were the third reason given for trying vaping after curiosity and because of use by a friend or family member.
Non-tobacco flavours preferred by young people are very similar to those preferred by adults. The most popular flavours used by adults are fruit, dessert, and other sweet flavours.
Restricting flavours would reduce appeal to adult smokers and would therefore result in a significantly more smoking. It would also lead to increased black-market supplies and home mixing, with little effect on youth uptake. One large study found that young people who started vaping with non-tobacco flavours were no more likely to go onto smoking than those who started with tobacco flavours.
According to Public Health England, “To date, there is no clear evidence that specific flavourings pose health risks but there are suggestions that inhalation of some could be a source of preventable risks”. These flavourings include diacetyl, cinnamaldehyde and benzaldehyde and should be avoided.
There is no evidence that nicotine causes harmful effects on the human adolescent brain.
Nicotine has been linked to harmful effects on the adolescent brain in animal studies. However, most animal studies use chronic, high-dose exposure to nicotine which does not accurately reflect the nicotine exposure that would occur from vaping in humans. The same effects found from nicotine in animals are also found in animal tests with caffeine.
Also, there is no long-term evidence of impaired brain function in the hundreds of millions of adults who smoked as adolescents and then stopped.
Nicotine in NRT is approved for use from the age of 12 in Australia.
A range of regulatory measures can be introduced to reduce uptake by young people as is the case with other adult products such as alcohol.
A ban is an unnecessarily restrictive policy. A ban will lead to a thriving black market for nicotine products and reduce access for smokers to a safer substitute. An appropriate regulatory policy should balance the needs of adult smokers and young people. Appropriate measures to protect young people include:
- Restrict sales of vaping products to specialist vape shops, pharmacies, adult stores and other suitable outlets and require strict proof of age at purchase points and via internet sales. Vaping products should also be available wherever tobacco is sold
- Maintain the current minimum age of sale for vaping products and e-liquids at 18 years and improve enforcement
- Consider access for selected young smokers with written permission of a parent or doctor
- Responsible advertising to adult smokers, avoiding any appeal to under 25s
- Packaging to restrict appeal to young people (images, colours, text)
- Restriction of e-liquid brand and flavour names which appeal to youth
- Child-resistant containers for e-liquid
- Further restrict access to smoked tobacco products, such as by reducing tobacco licences; enforcement of minimum age of sales; raise the age for tobacco sale to 21 years
Other issues
Vaping is largely confined to smokers and ex-smokers. Use by adults who have never smoked is rare.
In Australia in 2019, only 0.7% of never-smokers aged 14 and over were ‘current’ vapers (vaped at least once in the last 12 months). By comparison, 9.7% of smokers and 3.2% of ex-smokers vaped.
Some never-smoking vapers may have taken up smoking if vaping was not available.
Never-smokers who vape, also vape less frequently. Less than 0.3% of Australian never-smokers vape weekly or more. They are also less likely to use nicotine.
International surveys have found that vaping by adult non-smokers is generally <1%, for example England 0.4%; New Zealand no regular use; United States 0.3%; European Union current daily use by never smokers 0.08%; Germany 0.3%; Iceland 0.4%; and Greece 0.2%.
It is likely that these numbers will rise over time as some non-smokers who would otherwise have smoked are liable to take up vaping instead.
There is no evidence that vaping is renormalising smoking.
Vaping critics fear that widespread vaping could make smoking appear more socially acceptable again and undermine decades of successful tobacco control efforts. However, a review of studies on renormalisation found no evidence that this is happening.
According to Public Health England , ‘There is no evidence that ENDS are undermining the long-term decline in cigarette smoking among adults and youth and may in fact be contributing to it’. This was also confirmed in another study of adolescents in Great Britain during a period of rapid growth of vaping.
The main sign that renormalising is occurring would be stagnating or rising smoking rates. In fact, the opposite is occurring. Smoking rates have declined at a faster rate in the UK and US since vaping became widely available.
About one in two vapers also currently smokes (dual use). This is often a temporary transition phase and is usually less harmful than exclusive smoking. People vaping and smoking should be encouraged to quit smoking when possible.
Some smokers quit smoking soon after they start vaping. Others take longer and smoke and vape for a period while trying to transition to exclusive vaping.
Dual use tends to decrease over time as more dual users quit smoking. In Great Britain, 65.1% of vapers were also smoking in 2014. In 2020, the rate of dual use had almost halved to 38.3%.
In Australia, just over half of vapers are also smoking (54%). Smoking while using NRT is just as common as smoking while vaping, and is a transition towards quitting.
Dual users usually reduce their cigarette intake, often to very low levels because they are getting some of their nicotine from vaping. Most studies show dual users have lower levels of toxins in the body compared to exclusive smokers and many studies show improvements in health, such as blood pressure and asthma. However, when dual users do not reduce their cigarette intake, toxin levels are not reduced compared to smoking.
Dual users are more likely to quit smoking than other smokers, especially if vaping daily. However, dual users are more nicotine-dependent than exclusive smokers and many will not be able to quit smoking in a given attempt. Studies have typically found that 20-45% of dual users quit smoking over the next one to two years.
The only potential harm from dual use is if it reduces interest in quitting. However, this does not appear to be the case. Smokers who vape are more interested in quitting than those who do not and are more likely to make quit attempts.
Vaping is substantially cheaper than smoking and can lead to large financial savings.
Australia has the highest priced cigarettes in the world. A pack a day smoker currently pays $12,775 per year for a packet of cigarettes (20 Marlboro is $35) compared to around $1,500 per year for vaping, a saving of around $11,000 per year.
This is especially important for disadvantaged populations such as people with mental illness, substance use disorders, Indigenous people, homeless people and low-income groups whose families suffer considerable financial stress from smoking.
Disadvantaged populations have twice the smoking rate of the wealthy, smoke twice as many cigarettes and have lower quit rates. Smoking is a social justice issue and vaping could help reduce health and financial inequalities.
The precautionary principle is often invoked as a reason to delay the introduction of vaping because of uncertainties about future harm. However the precautionary principle is misused when applied to vaping in this way.
When correctly applied, the precautionary principle requires a full assessment of both the potential risks and benefits of both adopting and rejecting a new product.
In the case of vaping nicotine, the risks of NOT adopting vaping are much greater because cigarettes are substantially more harmful. Banning nicotine vaping denies smokers the opportunity to quit or switch to a much less harmful product.
This requirement for long-term evidence is not applied to other products. If we applied this standard in other areas, no new medicines would be introduced until we had safety data from 20-30 years of use.
Over the past 15 years there has not been a single confirmed death from nicotine vaping anywhere in the world and serious adverse effects are extremely rare. The alternative behaviour, tobacco smoking, kills 8 million people world-wide per year.
In Australia there are about 21,000 deaths each year from smoking related conditions.
The Royal Australian and New Zealand College of Psychiatrists states in its 2018 Position Statement on vaping:
“Further research is required to ascertain the effectiveness of e-cigarettes and vaporisers as tools for smoking cessation and whether they may provide a novel route into smoking initiation. This does not justify withholding what is, on the current evidence, a lower-risk product from existing smokers while such data is collected.”
The tobacco industry
The tobacco industry did not invent vaping and currently controls no more than 20% of the global vapour market.
Concerns about the tobacco industry’s agenda are understandable because of it’s appalling reputation. However, the reality is that vaping is a huge disruptive threat to the tobacco industry and is a direct competitor with tobacco sales. The tobacco industry began investing in vaping in 2012 in response to the clear threat and has been trying to catch up ever since.
As vaping has become more widespread, there has been an unprecedented decline in tobacco stocks. Share prices fell by more than half from 2017-2020:
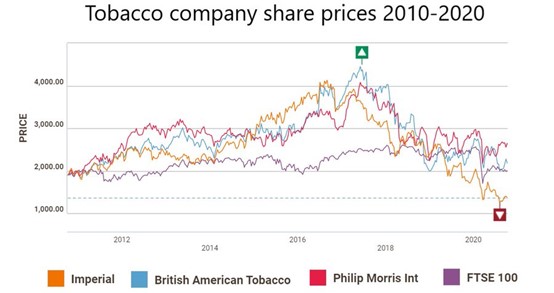
Conversely, proposals to restrict vaping are followed by a rise in tobacco stocks, for example here and here.
The primary focus should be on the improvement of public health. Safer alternatives to smoking will save lives, regardless of who manufactures them.
Furthermore, allowing reduced-risk options for nicotine may enable tobacco companies to escape from selling only the most dangerous options for delivering nicotine – combustible cigarettes.
Further reading
Mendelsohn CP. How opponents of vaping aid and abet Big Tobacco. The Spectator 2020
Regulation of vaping
An ideal regulatory approach should strike a balance between making high quality vaping products readily available to addicted adult smokers as a safer alternative while reducing access to young people.
Vaping products are classified as consumer products in other western countries, such as the UK, EU, New Zealand, Canada and US, ie as a safer alternative to another deadly consumer product, tobacco cigarettes. In Australia they are inappropriately classified as a poison or a therapeutic good.
Regulation of vaping should be proportionate to the risk of the product (the principle of proportionality). Vaping is at least 95% less harmful than smoking and should not be regulated like lethal tobacco products. Vaping does not involve tobacco, combustion or smoke and imposing harsh regulations that apply to tobacco is not appropriate.
Regulations on vaping should never be more restrictive than those for smoking. Vaping products should be at least as easy to access as cigarettes. The hardware, vaporisers, are currently regulated under consumer law.
Regulation of e-liquids should also ensure that high quality and safe products are available and includes:
- Exempt nicotine e-liquid in concentrations ≤ 5% for vaping from the Poisons Standard
- Regulate nicotine in concentrations ≤5% as a consumer product
- Minimise youth access by strict age verification, prohibited youth-friendly packaging, restricted advertising and public health messaging
- Introduce laws and guidelines specifying minimum standards for the manufacture and safety of vaping liquids
- Introduce mandatory standards for labelling, refill containers and health warnings
- Prohibit descriptive flavour names that specifically appeal to youth and unsafe flavouring chemicals
- Establish a notification scheme for pre-market registration
- Regulate and enforce the sale of nicotine e-liquids in vape shops, other retail outlets and online to under 18 year olds
- Permit vaping in specified public spaces and allow owners and managers of premises to set their own regulations
- Use public health messaging to raise awareness of the health risks relative to smoking tobacco
- Establish a system for reporting harmful effects and recall of unsafe products
Similar guidelines are currently successfully employed in the United Kingdom and are proposed for New Zealand.
Reading
Regulation of Nicotine E-liquids for Vaping in Australia. A discussion paper. ATHRA September 2020
Taxation on vaping products should be kept to a minimum to encourage smokers to switch to the safer product.
There is a good case for high tobacco taxes on cigarettes to discourage their use and reduce smoking rates. However, vapes are a less harmful substitute for smoking and there is no justification for high taxes on health grounds. Low taxes on vaping will provide an incentive to smokers to switch and will improve public health.
Vaping nicotine should be taxed according to risk in a similar way to nicotine replacement products. Vaping is at least 95% less harmful than smoking and is a lifesaving substitute behaviour.
Furthermore, smoking is increasingly concentrated in low-income and disadvantaged groups. A significant price advantage for vaping will incentivise low-income smokers to make the switch to the much less harmful alternative. A significant tax differential between vaping and smoking should be maintained.
One modelling study found that e-cigarette use is very responsive to price changes. Every 10% increase in e-cigarette prices was associated with a drop in e-cigarettes use by up to 11.5%.
High taxes on nicotine e-liquid were introduced in Italy in 2015 leading to the closure of 3 in 4 vape shops, the return of many vapers to smoking and growth in the black market. In 2018, the tax was cut by 80-90% and vaping started to increase.
Similar changes were found in Minnesota after tax rises on vaping were introduced.
Because the benefit to society is so high, regulators should look to other sources of income to replace tobacco taxes. Raising vape taxes to replace tobacco excise is as illogical as saying that someone who switches from driving a car to riding a bicycle should expect new taxes on biking to replace the lost petrol taxes.
Vaping products are consumer products and should be regulated by the Australian Competition and Consumer Commission (ACCC) which provide strong protection for consumers.
The ACCC ensures that products are safe, fit for purpose, of merchantable quality and comply with all legal requirements under the Competition and Consumer Act 2010.
Australian state and territory laws complement ACCC regulation of vaping products. They address the sale and supply of nicotine liquid, the sale of vaporisers, minimum age of sale, sale in vending machines, use in smoke-free areas, advertising and display. However, state laws are not uniform and a consistent national approach is needed.
Vaping products should not be regulated as they are at present by Australia’s medicines regulator, the Therapeutic Goods Administration (TGA). The TGA is responsible for regulating medicines and medical devices which make therapeutic (medicinal) claims, such as ‘this product can help you quit smoking’. Nicotine vaporisers are consumer products used almost exclusively as a less harmful substitute by smokers who can’t or won’t quit smoking or consuming nicotine.
No western country requires vaping products to undergo medicines regulation or a prescription. It makes no sense to require the highest standards of research and quality for nicotine vaporisers when they are replacing a far more harmful product, lethal cigarettes, which are virtually unregulated.
One practical outcome of TGA regulation would be the decimation of the vaping market. Every device and e-liquid and every future modification would require a detailed, costly and onerous application that only tobacco companies could afford. Most small to medium companies and vape shops would be driven out of business. The result would be that tobacco companies take over the vaping market.
New regulations to commence in 2021 will dramatically reduce access to nicotine vaping in Australia. Many vapers will go back to smoking or seek supplies from the black market.
Essentially, the proposed regulations require vapers to access nicotine liquid as a prescription medicine. However, there will be no product regulation and no manufacturing or safety standards which are required for all other prescription products.
The proposal makes it much harder to purchase vaping products than lethal cigarettes and will discourage smokers from switching to the much safer alternative.
Vapers don’t see themselves as sick and don’t want medical treatment. Doctors know very little about vaping and the Australian Medical Association opposes it. Few doctors will participate in the program. The Pharmacy Guild has stated that it will not support the sale of vaping products. The proposed process involves:
Licensed medical importers and pharmacy wholesalers source nicotine liquid from overseas
- Doctor applies online for approval to write nicotine prescriptions for vaping under the Approved Prescriber scheme
- Patient finds a doctor who will prescribe nicotine and gets a prescription if approved
Patient then either imports the nicotine e-liquid from overseas or purchases it from a local pharmacy. These steps are required for local purchase:
- Find a pharmacy which dispenses nicotine liquid and present the prescription
- Pharmacist orders the product from a wholesaler
- Patient returns to the pharmacist to purchase the product
Likely outcomes of the scheme are that:
- 42% of vapers will go back to smoking and 37% will get supplies from the black market according to a survey of nearly 7,000 vapers
- The cost of vaping products will increase substantially
- If Australia’s 520,000 vapers visit a doctor each year as advised, costs will range from $60-100 million per year for the taxpayer
- Vaping products remain totally unregulated, without safety standards, labelling, health warnings etc
- The range of nicotine liquids, flavours and prefilled nicotine pods will be greatly reduced
- Vape shops will be decimated. Vape shops play a valuable role in helping smokers to quit. Staff are former smokers who vape and can give invaluable advice and support.
The Health Ministers plan to ban personal importation of nicotine by changes in Customs Regulations has been deferred for a second time in October 2020. The future of this draconian plan is unknown.
Further reading
Government delivers another knockout punch to vapers. ATHRA 23 September 2020